
Micronutrients
Where To Get Key Nutrients:
Vitamin A
Liver
Egg yolks
Extra virgin cod liver oil
Vitamin C
Citrus fruits
Bell peppers
Dark leafy greens
Kiwi
Broccoli
Berries
Tomatoes
Papaya
Brussels sprouts
Cantaloupe
Vitamin D
Extra virgin cod liver oil
Cold water, fatty fish – salmon, sardines, mackerel
Shellfish – oysters, clams, shrimp, etc.
Vitamin K2
Grass-fed dairy
Poultry liver
Natto: fermented soybeans
Magnesium
Dark leafy greens
Nuts and seeds – especially pumpkin seeds
Cold-water fatty fish
Avocados
Yogurt
Bananas
Dark chocolate
Molasses
Figs
Iodine
Seaweed
Cold-water fatty fish
Shellfish
Potatoes
Cranberries
Organic dairy products
Micronutrients
Biotin (B7)
FUNCTION
- Activates the enzymes called carboxylases. These enzymes are involved in fatty acid synthesis and breakdown, cellular energy metabolism, and ketone body production.
DEFICIENCY/TOXICITY
- Overt biotin deficiency in children and adults is rare and is usually due to genetic inborn errors of metabolism. However, up to half of pregnant mothers in the United States may have mild biotin deficiency.
- Symptoms of biotin deficiency include depression, fatigue, hallucinations, hair loss, numb or tingling sensations in the arms and legs, and a red, scaly rash around the eyes, nose, and mouth.
- Biotin deficiency may also contribute to birth defects during pregnancy.
- Avidin, a protein in egg whites, can also bind biotin, so high consumption of raw egg whites significantly increases the risk of biotin deficiency. Heating egg whites decreases the amount of this protein, but some of it will remain in cooked eggs.
- Other risk factors for biotin deficiency include chronic alcoholism and chronic antibiotic use.
- There are no reported toxicities of biotin. However, very high intake of biotin may interfere with diagnostic assays that use biotin technology, such as those commonly used to measure thyroid hormones and 25-hydroxyvitamin D. Even a single 10 mg dose of biotin interferes with thyroid function tests, and there are several cases of patients being misdiagnosed with hyperthyroidism due to high-dose biotin supplements.
BEST FOOD SOURCES
- Liver, eggs, fish, pork, beef, peanuts, almonds, sunflower seeds, sweet potatoes, spinach, broccoli, and other vegetables. It is also found in dairy products.
RECOMMENDED DAILY ALLOWANCE (RDA)
- Biotin is not stored in large amounts in the body, so we need a regular supply of biotin.
- Adults require an estimated 30 mcg of biotin per day.
NOTES
- The gut microbiota also contributes some biotin, but the exact amount is unknown.
- If biotin deficiency is suspected, we should first remove any raw egg whites from the diet and encourage increased consumption of liver and egg yolks.
- Supplementing biotin can be used quite safely either on its own or as part of a B-complex if other B vitamin deficiencies are present.
Calcium
FUNCTION
- Vitamin D, Calcium, and Phosphorus must be considered together
- Main structural component of bone and teeth
- Plays a role in cell signaling
DEFICIENCY/TOXICITY
- Poor bone density – osteopenia, and osteoporosis
- Can be from low calcium, elevated parathyroid hormone (PTH), or excess phosphorus
- Osteomalacia (softening of the bones from impaired bone metabolism)
- Rickets is the childhood version
- Can be caused by low calcium, phosphorus, and/or vitamin D
- Tetany (muscle twitching, tremor, spasms, confusion, and in severe cases seizures, coma and death)
- Can be caused by deficiency of vitamin D or calcium, or a large excess of phosphorus
- Soften tissue calcification which can cause kidney stones and cardiovascular disease
- Can be caused by deposits of calcium that was not transported to the bone
- Excess of vitamin D, calcium, and phosphorus
- Frequent thirst and urination, confusion, lethargy, fatigue, depression, bradycardia (slow heart rate), arrhythmia, palpitations, or fainting
BEST FOOD SOURCES
Sesame seeds, bone-in fish (sardines, salmon), dairy, dark leafy greens (collards, turnip greens, kale, bok choy), broccoli, cauliflower
RECOMMENDED DAILY ALLOWANCE (RDA)
- 1000-1200 mg/day (adults)
- A Paleo-type diet may also lead to increased absorption.
- Remember that vitamin D is required for optimal calcium absorption.
- Higher-protein diets can also increase the absorption of calcium, and high levels of calcium supplementation can lead to hypercalcemia, which can be fatal if left untreated.
NOTES
- Calcium levels are tightly regulated in the body by parathyroid hormone and vitamin D, and if intake of calcium is not high enough, levels are maintained at the expense of bone health.
- The absorption of calcium from plant foods is generally lower than it is from animal foods.
- Vitamin D increases intestinal absorption of calcium, helps maintain levels in the blood and enables the proper mineralization of bone.
- Vitamin K2 activates osteocalcin which regulates calcium metabolism via carboxylation. Carboxylated osteocalcin deposits calcium in bones and the teeth and keeps it away from the soft tissues.
- High sodium excretion can lead to higher levels of calcium excretion in the urine.
- Niacin (B3) plays a role in the mobilization of calcium.
- Calcium can inhibit the absorption of heme iron.
- Calcium supplements do not reduce fracture rates and may even increase them. While calcium is a crucial mineral for us, supplemental calcium has been shown to increase the risk of cardiovascular disease and cardiovascular events. It is thought that supplemental calcium promotes calcification or hardening of the arteries, so it is important to make sure that people are taking vitamin K2 and consuming enough vitamin A and also ensure that vitamin D levels are adequate. All of these will have an effect on calcium metabolism.
- Whole bone calcium is a good option for supplementation. Whole bone calcium would be expected to affect the body in much the same way that dietary calcium would, rather than how calcium supplements do.
Choline
FUNCTION
- Vitamin-like nutrient that is essential for proper growth, development, and function of the human body
- It is a component of phospholipids, which make up the structure of cell membranes
- It is a precursor to the neurotransmitter acetylcholine, which plays roles in memory, circadian rhythms, and motor control, and a precursor to sphingomyelin, which is found in the fatty sheath around nerve fibers and improves the conduction of electrical impulses
- The transport of fat and cholesterol from the liver also requires choline as a component of lipoproteins
- Choline is an important source of methyl groups, so it plays an important role in epigenetics
- Epigenetics are modifications on top of the underlying DNA structure but do not alter the actual DNA sequence
- Epigenetics play an important role in health throughout life but are particularly important during growth and development as fetal stem cells divide and differentiate into organs with many different complex functions
- During pregnancy, maternal choline status also has implications for the structural development of the hippocampus, the primary brain region responsible for learning and memory
BEST FOOD SOURCES
Animal products such as beef liver, eggs, muscle meat, and fish provide the largest amount of dietary choline. Plant foods such as shitake mushrooms, potatoes, Brussels sprouts, and broccoli also provide some choline.
RECOMMENDED DAILY ALLOWANCE (RDA)
There is no active consensus on how much dietary choline we actually need. The Institute of Medicine has resorted to establishing adequate intake values, since there is insufficient evidence to establish an RDA for choline.
Adult men are estimated to require 550 mg of choline per day, while adult women need an estimated 425 mg per day, with needs increasing during pregnancy and lactation.
NOTES
- Genetic variants such as PEMT and MTHFR mutations, a high overall energy intake, and low intake of other methyl donors will all increase the need for choline
- Choline needs depend on the gut microbiome
- A recent study suggests that microbes in the small intestine compete with the host for choline absorption. This suggests that those with gut dysbiosis or SIBO could have symptoms of choline deficiency even if they are consuming adequate dietary choline or taking supplements
- According to a recent estimate, nine out of 10 Americans do not get enough choline
- Choline deficiency can cause muscle damage, liver damage, and nonalcoholic fatty liver disease. It may also cause changes in DNA methylation
- Altered DNA methylation has been associated with cancer, aging, cognitive impairment, autoimmunity, and atherosclerosis
- Up to 95 percent of pregnant women consume less choline than they need
- Poor maternal choline status has been associated with an increased risk of neural tube defects and altered development of the hippocampus
- One of the most important roles of choline in physiology as a methyl donor first requires its conversion to betaine. Since choline has several functions besides methylation, betaine cannot completely fulfill choline requirements. However, adequate betaine can help prevent some of the consequences of choline deficiency. Betaine may also be more likely to be absorbed in those who have small intestinal dysbiosis, or SIBO
- Choline can also be taken safely as a supplement in the phosphatidylcholine form. It is important to note that most prenatal supplements and multivitamins do not contain choline, and those that do often contain the choline chloride form, which is not as bioavailable
- Those with SIBO can also consider supplementing with betaine HCl. This is typically used to help restore adequate stomach acid, but it may also help protect against choline deficiency
Chromium
FUNCTION
- Chromium supports glucose tolerance and insulin sensitivity. It is required for glucose transport into cells. It improves cell wall sensitivity to insulin. The mechanism is that it upregulates insulin signaling molecules, which in turn may increase glucose transporters. So more glucose ends up in the cell where it can be converted to energy, instead of hanging out in the blood increasing blood glucose levels.
- Chromium also supports increasing HDL cholesterol in several small studies. HDL cholesterol is considered the healthiest version of cholesterol. Additional research needs to verify the above in larger human trials and to better understand other possible roles of chromium. A few human studies suggest chromium supplementation may support those who already have type 2 diabetes with the actions already mentioned above. But this has not been shown to prevent type 2 diabetes in those who don’t have it. The effect on helping improve type 2 diabetes is small, but considered statistically significant.
DEFICIENCY/TOXICITY
- Type 2 diabetes was an outcome of a patient on total parenteral nutrition (IV feedings). This was reversed when chromium, initially absent from the TPN formula, was added back in, in a matter of weeks. Severe neuropathy was also seen in the above patient that was fully reversed with added chromium. Chromium may be associated with diabetes based on current evidence we have from small trials, as I already mentioned.
- High levels of environmental exposure from inhalation of industrial dust are associated with lung cancer and dermatitis.
- There is little evidence for oral toxicity.
- The Food and Nutrition Board at the Institute of Medicine did not set a tolerable upper limit of chromium at this time due to no concrete evidence of toxicity from oral intake. However, keep in mind that based on cell culture studies, high level intakes considered greater than 300 micrograms per day may cause oxidative damage to cells.
BEST FOOD SOURCES
- The highest concentrations are found in egg yolks, whole grains, unrefined sugars, and brewer’s yeast, but not other edible types of yeast.
- There are some foods that also provide lower amounts of chromium. These include fruits, especially grape juice, apple with the peel, and bananas. Vegetables can be a good source, especially green beans and broccoli and potatoes, as well as meat, coffee, and nuts.
RECOMMENDED DAILY ALLOWANCE (RDA)
- We do not have enough data to establish an RDA for chromium, so adequate intake levels were established by the Food and Nutrition Board at the Institute of Medicine. But to give you a general idea, female adults need an estimated 20 to 25 micrograms per day, and male adults need an estimated 25 to 35 micrograms per day.
- Early research suggests that needs for chromium likely coincide with carbohydrate intake. The more carbohydrates consumed, especially the refined and processed types, the more chromium is likely needed based on the known action of chromium.
- Here’s a quote from findings of a study published in Diabetes Journal in 1997: “The beneficial effects of chromium in individuals with diabetes were observed at higher levels than the upper limit of the adequate intake.” This was a study involving 180 men and women with type 2 diabetes, taking normal medications, no changes in dietary intake or living habits, who were supplemented with 1.5 milligrams, or 150 micrograms, who saw statistically significant improvements in hemoglobin A1c, fasting glucose and a two-hour postprandial glucose at the two-month and four-month mark. Cholesterol numbers also improved in these subjects.
- Many Functional Medicine providers are supporting chromium supplementation in those with uncontrolled type 2 diabetes at levels between about 200 and 300 micrograms per day, either individually or in a blend of blood glucose-supporting nutrients. At this time, no adverse effects have been seen. Note, however, that individuals with type 2 diabetes require careful monitoring by a clinician.
NOTES
- Chromium competes for a binding site on an iron transporter called transferrin. When iron is high, as in iron overload or hemochromatosis, this may lead to low levels in chromium that may contribute to insulin resistance and increased glucose levels.
- Vitamin C intake with chromium increased absorption and plasma levels of chromium in one small human study.
Cobalamin (B12)
FUNCTION
- B12 is heavily involved in metabolism in every cell in the human body
- It is a vital nutrient cofactor required to make our DNA
- It is critical for how we process fatty acids and amino acids
- Tied to making all new things like skin, collagen, and red blood cells and creating energy
- B12 is required to make myelin, the protective insulation around our nervous system
- It is required for the proper growth and development of red blood cells needed to carry oxygen for our body
- B12 works with folate (B9) to support red blood cell production
- Vitamin B12 deficiency causes the same macrocytic megaloblastic anemia that folate deficiency causes
- Macrocytic means cells that grow larger and don’t divide and separate into two cells, like they’re supposed to
- Megaloblastic means abnormally large, immature, and dysfunctional red blood cells
- High folate intake can mask vitamin B12 deficiency
- Vitamin B12 deficiency causes the same macrocytic megaloblastic anemia that folate deficiency causes
- Vitamin B12 also works together with folate (B9) to support methylation
- Methylation prevents rumination on negative thoughts and emotions
- Keeps our histamine levels low to prevent allergy-type symptoms
- Boosts choline to protect against fatty liver
- Support digestion of fat
- Sustains attention and memory
- Helps make creatine to support building and keeping muscle for healthy digestion and positive mood
BEST FOOD SOURCES
- Food sources are primarily animal-based
- Vegan or vegetarian food plan do not get a lot of animal-based foods are especially at risk of vitamin B12 deficiency
- Liver, oysters, nori, meat, poultry, fish, milk, cheese, mushrooms – especially black trumpet, chanterelle, or shiitake mushrooms.
- Eggs are not a really good source of vitamin B12.
- People who are lacto-ovo vegetarians that don’t eat nori or mushrooms and rely on milk only for their vitamin B12 might be at risk for vitamin B12 deficiency
- Omnivores may be compromised unless you eat liver, oysters, clams, or at least 12 ounces of meat, poultry, fish, or dairy each day
RECOMMENDED DAILY ALLOWANCE (RDA)
2.4 mcg/day – adult
NOTES
- Water-soluble vitamin
- B12 is the largest and the most complex B-vitamin
- What can cause B12 deficiency?
- Low levels of stomach acid
- Poor intake due to low intake of animal products
- Celiac disease or other gastrointestinal diseases that interfere with absorption
- A parasitic infection of the gut
- Malabsorption caused by certain medications such as metformin, alcohol, proton pump inhibitors, and antihistamines
- Chronic pancreatitis
- Resection (removal of a portion of either the large intestine or small intestine)
- Poor absorption is the main reason for deficiency
- One possible cause is an H. pylori overgrowth causing inflammation or gastritis
- Celiac disease or SIBO may also interfere with absorption
- An autoimmune condition can interfere with the ability to bind and carry B12 to the ileum, the lower part of the small intestine, where it is absorbed
- Low vitamin B12 causes low pantothenic acid (B5)
- When both B12 and B5 are low, toxic amino acid breakdown products can’t be properly methylated and can cause memory loss, mood and behavior changes, and even possible delirium or psychosis
- Common signs of vitamin B12 deficiency that start in the feet and work their way up the body:
- A sense of body position or strange walking gait happen
- Tingling, numbness, or feeling of something crawling in your skin, especially toes, lower legs, hands and arms
- Poor control or loss of control of movements
- Poor ability to relax muscles
- Visual disturbances, dizziness, faintness upon standing, and this is related to sudden changes in blood pressure
- Select exercise intolerance
- Poor energy or fatigue
- Greater than 70 percent of all vegetarians and greater than 90 percent of all vegans have evidence in bloodwork of early vitamin B12 deficiency
- When supplementing with vitamin B12, be aware of different forms and methods and forms of supplementation:
- Methods:
- Oral
- Intranasal spray
- Injections
- IV therapy
- Forms:
- Natural: Methylcobalamin, adenosylcobalamin, and hydroxocobalamin
- Synthetic: cyanocobalamin
- Methods:
Copper
FUNCTION
- Copper is a trace mineral that is essential to all living organisms. In the mitochondria, copper is a key component of cytochrome c oxidase, which catalyzes the last step in the electron transport chain, reducing oxygen to water.
- Copper is also crucial for the function of superoxide dismutase, an antioxidant enzyme that helps to detoxify free radicals.
- In humans, copper is primarily found in muscle, liver, and bone.
DEFICIENCY/TOXICITY
- Copper deficiency can cause anemia, and deficiency of copper can also impair iron absorption itself.
- Low copper can also cause hypopigmentation of hair and skin, hyperthyroidism, and neurotransmitter and endocrine imbalances such as high serotonin and low adrenaline.
- Other signs and symptoms of copper deficiency include high leukocyte and neutrophil counts, osteoporosis, and histamine intolerance.
- Copper deficiency can also cause abnormalities in glucose and cholesterol metabolism.
- Risk factors for copper deficiency include high-dose zinc supplementation, impaired methylation, small intestinal malabsorption disorders, and the use of proton-pump inhibitors and antacids.
- The ratio of dietary zinc to copper should be kept between 2:1 and 15:1 for optimal health.
- The only established syndrome of copper toxicity in the literature is Wilson’s disease, which is a genetic condition characterized by an inability to excrete copper. As a result, copper accumulates in the body and is deposited in the cornea, liver, and brain. Wilson’s disease requires chelation therapy under close medical supervision. In those without Wilson’s disease, excess copper may cause oxidative stress and is thought to potentially play a role in neurodegenerative diseases such as Alzheimer’s, behavioral diseases such as ADHD, depression, and even paranoid schizophrenia.
- High copper can also cause estrogen imbalance, which can potentially lead to skin issues, headaches, poor immune function, and severe PMS.
- The Institute of Medicine has set the tolerable upper limit for copper intake at 10 mg per day. Diets high in copper are unlikely to meet this upper limit and will also contain zinc, which protects against copper toxicity.
RECOMMENDED DAILY ALLOWANCE (RDA)
Adult men and women require 900 mcg of copper per day.
BEST FOOD SOURCES
Oysters, beef liver, dark chocolate, sunflower seeds, lentils, mushrooms, almonds, turnip greens, asparagus, blackstrap molasses
NOTES
- Copper deficiency can impair iron absorption; zinc balance
- Supplementation: 3 to 7 mg per day to correct deficiency.
- If supplementing with copper, blood levels of zinc and copper should be monitored closely by a healthcare practitioner.
- Infants cannot regulate the absorption of copper and should never be given copper supplements. On the other hand, if copper is too high, we want to limit copper intake from foods and reduce exposure to copper in the environment from copper pipes and copper cookware.
- Women with excess copper may also want to consider alternatives to copper IUDs.
- Improving zinc status can also help protect against copper toxicity.
Folate (B9)
NAMES
Folate, folic acid (synthetic form), vitamin B9, 5-MTHF (5-methyltetrahydrofolate)
FUNCTION
- Necessary for dopamine production
BEST FOOD SOURCES
Foods that are naturally rich in folate include liver, spinach, lentils, collards, broccoli, beets, cauliflower, parsley, mustard greens, turnip greens, and some lettuce.
RECOMMENDED DAILY ALLOWANCE (RDA)
400 mcg/day – adult
600 mcg/day – pregnant
500 mcg/day – lactation
NOTES
- Folate deficiency can decrease serotonin synthesis, s-adenosylmethionine (SAM), and increases inflammatory homocysteine; is associated with depression, epilepsy, psychiatric conditions (especially in the elderly)
- There is a possible link between folate and homocysteine levels and aging, dementia, and Alzheimer’s disease
- Folic acid is an oxidized synthetic compound used in most dietary supplements and food fortification.
- It was introduced into the food supply to reduce the risk of neural tube defects during malnourished pregnancies.
- It can be converted into folate, which is the active form of the nutrient that is used in the body, but that conversion is limited in humans.
- Low conversion of folic acid to folate can lead to high levels of unmetabolized folic acid in the systemic circulation. High levels of unmetabolized folic acid in the bloodstream can cause problems.
- It masks vitamin B12 deficiency, which may lead to deterioration of the central nervous system, especially in the elderly.
- It causes anemia and cognitive impairment.
- It speeds up progression of certain cancers, including colon and prostate cancer.
- It depresses immune function and is associated with increased all-cause mortality.
- If you are supplementing, make sure you are taking one of the natural forms of folate:
- 5-methyltetrahydrofolate (5-MTHF)
- Metafolin
- Folinic acid
- If pregnant, make sure your prenatal not only has a natural form of folate, but also make sure there’s a minimum of 400 mcg
Inositol (B8)
FUNCTION
- Inositol is a type of sugar that mediates cell signaling for some hormones, neurotransmitters, and growth factors.
- The main use of inositol is for the storage and metabolism of amino acids. It is also an important part of the citric acid cycle, or the main series of chemical reactions that leads to food being turned into energy within the body.
- Inositol benefits the immune system and the production of hair and nails.
- It will help with insulin sensitivity and may also help with the decrease in the androgens and the shift to estrogens.
- Benefits include supporting symptoms of mental health conditions such as panic disorder, depression, anxiety, obsessive-compulsive disorder, and bipolar disorder. Additional benefits include supporting PCOS, blood pressure issues, elevated blood lipids, working toward improved fertility, and better embryo quality.
BEST FOOD SOURCES
Food sources include brewer’s yeast, cabbage, cantaloupe, chickpeas, lima beans, unrefined molasses, nuts, raisins, wheat germ, whole grains, citrus fruits (except for lemons).
RECOMMENDED DAILY ALLOWANCE (RDA)
- 1-3 grams to improve REM sleep
- 100mg to strengthen the liver
- 1000-2000mg/day for PCOS
NOTES
- Examine points out that inositols are pseudovitamin compounds that falsely belong to the B complex family. Its actions mimic those of some B vitamins, and that is why we call it a vitamin B-like substance.
- There are nine forms of inositol overall. Specifically, myo-inositol (MYO) and d-chiro-inositol (DCI) are two forms that have been studied for their abilities, especially towards women with polycystic ovary syndrome (PCOS) when it comes to properly utilizing insulin and helping preventing insulin resistance. Every tissue in the body has its own ratio of MYO to DCI, with the former having higher amounts and producing DCI when needed.
- D-chiro-inositol isn’t naturally abundant in food, since the human body makes it from myo-inositol through the actions of an enzyme called wpimerase.
- Myo-inositol has also shown promise for anxiety by working as an antidepressant and helping alleviate conditions such as panic disorders and binge eating.
- Inositol benefits other conditions as well, such as:
- Diabetic nerve pain
- High cholesterol levels
- Insomnia
- Alzheimer’s disease
- ADHD
- Psoriasis
- Autism
- Hair growth
Iodine
FUNCTION
- Required to make thyroid hormone, both T4 and T3
RECOMMENDED DAILY ALLOWANCE
- The RDA for iodine for adults is 150 mcg per day, 220 mcg a day for pregnant women, and 290 mcg a day for breastfeeding women.
- During pregnancy and breastfeeding, infants are completely reliant on the mother’s store of iodine, so it is especially important to make sure pregnant and lactating mothers are getting enough.
- The World Health Organization estimates that over 30 percent of the world’s population is iodine deficient. However, this is less likely in countries with iodized salt, though it is more common than you might think in developed countries.
BEST FOOD SOURCES
Sea vegetables (esp. kelp and kombu), saltwater fish, eggs, cheese
- Sea vegetables such as kelp, kombu, hijiki, arame, and dulse are by far the highest sources of iodine. A single gram of kelp contains over 1,000 percent of the daily value of iodine that you need.
- Iodine content can vary by each type of seaweed, and cooking does cause seaweed to lose quite a bit of its iodine. For example, boiling kombu will destroy about 99 percent of its iodine. However, because these sea vegetables are so rich in iodine, even if 99 percent is destroyed, they will still contain significant amounts of iodine.
- Other good sources include commercial dairy and some bread products where iodine is added.
- The easiest way to get more iodine is to use kelp flakes, which you can buy at most health food stores or online, in place of sea salt. They are great on eggs, in soup, or any other food that you put salt on. Just one-quarter teaspoon a day of kelp flakes would more than satisfy your daily need for iodine. Use kombu to flavor soups or stews. You can add one 4- to 6-inch piece, about 6 g, to a soup, about 15 minutes before it is finished. Eat seaweed as a snack or a side dish. There are many seaweed snacks available now. Of course, sushi or nori rolls, although note that nori is the lowest in iodine among the seaweeds.
NOTES
- The thyroid gland of a healthy adult contains about 70 to 80 percent of the total body iodine.
- Iodine deficiency is recognized as one of the most common preventable causes of brain damage. It can cause mental retardation, goiter, and other growth and developmental problems.
- One of the first signs of iodine deficiency is goiter, which is swelling of the thyroid gland. Iodine deficiency can also cause hypothyroidism. In fact, it is the second most common cause of hypothyroidism behind autoimmune Hashimoto’s.
- In an effort to combat iodine deficiency, many developed countries such as the United States started iodizing salt, but a lot of health-conscious clients will use sea salt instead of table salt, which does have a lot of benefits, but it does not contain significant amounts of iodine.
- I recommend a maintenance dose of iodine of about 800 mcg to 1 mg a day.
- The upper limit for iodine is set at 1,100 mcg per day for adults. However, that does not apply for people who are being treated with iodine under medical supervision. There are two groups of people who getting the right amount of iodine is absolutely crucial for: people with hypothyroidism, and pregnant and breastfeeding women.
- You may have heard that iodine can be problematic for people with Hashimoto’s, and there is some research to support that. However, the research suggests that it is far less likely that someone with Hashimoto’s will react to iodine supplementation if they are also getting enough selenium in the diet. Those with hypothyroidism should probably work with a licensed practitioner to determine their ideal iodine and selenium intake.
- Iodine deficiency can cause hypothyroidism in both the mother and the fetus. Maternal hypothyroidism has been associated with increased risk for preeclampsia, miscarriage, stillbirth, preterm birth, and low birth weight infants. Additional iodine is needed during pregnancy and lactation because of increased thyroid hormone production and the transfer to the fetus before the fetal thyroid gland is developed, increased urinary excretion of iodine, and increased iodine transfer to the infant during breastfeeding.
- Caution with higher doses of iodine with people on Coumadin, as that may decrease the anticoagulant properties of that drug. Otherwise, iodine has very few interactions with medications.
Iron
FUNCTION
- Iron is part of many enzymes and proteins in the body.
- It is found in foods as heme and non-heme iron.
- Heme iron is found in meat, poultry, and fish. Despite being only 10 to 15 percent of the iron found in food, it makes up about one-third of what we absorb.
- Non-heme iron is found in plants, dairy products, and in some meats as well. Unlike heme iron, non-heme iron absorption is greatly influenced by food components in the same meal. These include enhancers such as vitamin C and other acids, as well as sources of heme iron and inhibitors such as phytic acid, polyphenols, and soy protein.
BEST FOOD SOURCES
Clams, oysters, beef, chicken liver, lamb
RECOMMENDED DAILY ALLOWANCE (RDA)
The RDA is 8 milligrams, except for menstruating females, for whom it is 18 milligrams. This increases to 27 milligrams a day when a woman becomes pregnant.
IRON OVERLOAD / HEMOCHROMATOSIS
- Too much iron is not a good thing. There’s a disorder called hemochromatosis, which is a genetic disorder that is characterized by excess iron storage.
- Hemochromatosis is associated with a huge range of chronic conditions —everything from Alzheimer’s and dementia to diabetes and metabolic syndrome to inflammatory bowel disease, gout, osteoarthritis, and all kinds of neurological disorders.
- Even mild iron overload can cause increased mortality and morbidity, so early death and disease. Like hemochromatosis, it is associated with metabolic, cardiovascular, and neurodegenerative problems, although not to the same degree.
- Iron overload is highly correlated with impaired glucose tolerance. Clients with metabolic issues should be checked for iron overload by a healthcare practitioner.
- Iron overload can reduce insulin synthesis and secretion. It can decrease insulin sensitivity in the liver, and iron deposits in the liver can decrease glucose uptake, thereby increasing someone’s risk of diabetes.
- When you see markers out of line, retest and then check genetics for predisposition to hemochromatosis.
- Treatment for iron overload is usually regularly scheduled phlebotomy if the person has hemochromatosis or just donating blood if it is a mild version of iron overload. Lactoferrin, which is a supplement, can also be used to remove iron from tissues that are already loaded with iron.
- People with hemochromatosis should not take supplements that contain iron. They will have been advised of this by their healthcare practitioner. They would want to limit or possibly avoid foods that are extremely high in iron, such as clams, chicken liver, oysters, octopus, and beef liver. Usually these people will be able to tolerate some amount of meat, such as regular ground beef and things like that without too much trouble. But that is something they’ll have to discuss specifically with their clinician.
- They would also want to avoid things that enhance the absorption of iron.
- Alcohol, supplemental vitamin C, betaine hydrochloric acid, zinc, and beta-carotene can all increase the absorption of iron. On the other hand, there are several things that can inhibit the absorption of iron. Tannins, like in tea and coffee, will inhibit non-heme iron absorption.
- Almost everything that we’re talking about only inhibits plant-based forms of iron, except for calcium. Oxalic acid, found in sweet potatoes, spinach, and so on; eggs; food with phytic acid, such as greens and nuts; phosphates—all of those can inhibit the absorption of non-heme iron. Only calcium inhibits heme iron absorption from animal products and non-heme iron absorption. The best way to do that is with dietary calcium, like in dairy products or bone-in fish. Supplemental calcium, when used in higher doses, is problematic.
Magnesium
FUNCTION
- Magnesium is vital to the human body. Over 300 enzymes need it, including every enzyme involved with ATP and enzymes involved in DNA and RNA production.
- It plays an important role in bone health, and most of the body’s magnesium is, in fact, stored in bone, more than 60 percent of it.
- Magnesium also helps transport ions across the cell membrane surface.
DEFICIENCY/TOXICITY
- Most Americans are deficient in magnesium, though there are certain conditions that make deficiency more likely, such as digestive disorders like inflammatory bowel disease or GERD, especially if they are taking PPIs; renal disorders; alcoholism; and older age.
- Median intake of magnesium is well below the RDA. It can be difficult to get enough magnesium in the diet for a few reasons. First is that soils have become progressively depleted in magnesium, and secondly, anti-nutrients such as phytic acid can inhibit the absorption of magnesium.
- Magnesium deficiency can cause many symptoms, including muscle cramps, heart arrhythmias, tremor, headaches, and acid reflux. It is also associated with cardiovascular disease, high blood pressure, metabolic syndrome, diabetes, migraines, PMS, asthma, and hypothyroidism.
- Given magnesium’s vital role in the human body, it is easy to see why deficiency can cause such widespread problems. If you have any of these conditions, you will likely do very well with magnesium supplementation and/or increasing intake in the diet.
- Unless you are actively aware of your magnesium intake, you can pretty much assume that they are not getting enough. The optimal range is 500 to 700 mg per day from a combination of food and supplements.
- Given this, many people will need to supplement to get adequate magnesium. The average American gets less than 250 mg per day from the diet, while people on a more nutrient-dense diet such as a Paleo-type diet probably get closer to 350 to 400 mg. The range of supplementation could be between 100 to 500 mg a day depending on your background intake.
- I prefer magnesium glycinate or malate because I have found that they are better absorbed than most other forms of magnesium such as oxide, orotate, or citrate.
RECOMMENDED DAILY ALLOWANCE (RDA)
RDA of 400 to 420 mg for adult men and 310 to 320 mg for women.
BEST FOOD SOURCES
- Food sources of magnesium include nuts such as pumpkin seeds and almonds, but phytates, or phytic acid, in nuts inhibits the absorption of magnesium. To mitigate these effects, soak and then dehydrate or roast your nuts or seeds before consuming them in order to remove the phytic acid and allow better absorption.
- Other high-magnesium foods include dark leafy greens such as spinach and chard, molasses, bananas, and yes, dark chocolate. Chocolate is a legume, so it does have phytic acid, which would inhibit absorption, but it is generally fermented during the preparation of chocolate products, so I think a pretty good amount of magnesium will be absorbed from dark chocolate. Legumes can also be a good source of magnesium if the client tolerates them, but like nuts, they need to be properly prepared, meaning soaked, in order to remove the antinutrients that can block the magnesium absorption.
NOTES
- Magnesium has been shown to be better absorbed with a higher protein intake.
- Magnesium can also interfere with the following drugs: digoxin, which is a heart medication; nitrofurantoin, which is an antibiotic; certain antimalarial drugs or bisphosphonates for osteoporosis.
- The side effects of too much magnesium can include loose stools.
Manganese
FUNCTION
- Manganese is an essential mineral. It’s elemental symbol is Mn.
- It’s a very important antioxidant, as MnSOD which stands for manganese superoxide dismutase. The mitochondria, where energy is made in every cell in our body, can easily be damaged by oxidative stress. Interesting to know that every time we make a molecule of ATP, or energy, in the mitochondria, we also make a superoxide free radical. If we can’t degrade that superoxide, it can build up and harm our mitochondria and ourselves. You can see that manganese is important to protect our ability to make energy. While hydrogen peroxide isn’t that great for the body either, it’s better than superoxide, and our body has another great mechanism built in to help degrade hydrogen peroxide in another step.
- Manganese is an important activator for many enzymes that help metabolize carbohydrates, proteins, and fats.
- One example is that it helps mop up ammonia made when we degrade protein.
- Another is activating the conversion of glutamate to glutamine. If glutamate builds up, it is neurotoxic and inhibits the calming neurotransmitter GABA.
- Manganese assists with the healthy formation of bones and cartilage.
- It supports wound healing by helping form new collagen and skin cells.
DEFICIENCY/TOXICITY
- Deficiency is less common than toxicity. However, it can happen. Here’s a list of some signs of manganese deficiency:
- Poor bone health or formation could look like osteoporosis, or poor skeletal growth in a child, for example, or a skin rash that is called miliaria crystalline on the torso, which looks like red little blisters that become really scaly with healing. Another is low cholesterol, impaired glucose tolerance, slowed growth, such as hair and nails, especially, impaired reproductive function, more pronounced premenstrual syndrome symptoms, low energy, weight loss, and poor ability for wound healing.
- Toxicity with manganese usually occurs from high environmental exposures, and it’s not really that common. But it could happen with inhaled manganese, such as a welder might be inhaling manganese dust or ingested manganese as with a possible source of contaminated water.
- There is one clinical case of oversupplementation. It’s recorded based on a person who took large amounts in supplement form for years. What kind of symptoms do we see when this happens? They’re pretty severe. Gradual neurological damage that may lead to Parkinson’s disease, tremors, and spasms. May include psychiatric symptoms like irritability, aggressiveness, and even hallucinations. Inflamed lungs can occur that include a cough, acute bronchitis, and poor lung function. We’ve also seen cognitive and behavioral deficits that can occur in children when exposed from drinking water. Keep in mind that manganese toxicity from foods alone has no record of being documented in humans.
- Consider supplementing on the advice of a healthcare provider who can assess your symptoms and/or test your levels. A carnivore-based food plan with little or no plant food might need supplementation. But remember, spices are a great source.
- Do not supplement if you have iron deficiency because harmful levels of manganese can reach your brain.
- Do not supplement with infants, during pregnancy, or breast-feeding.
- Avoid with chronic liver disease. The liver may struggle to eliminate any excess leading to toxicity. That said, if someone supplements, this should be limited to no more than 3 milligrams per day.
RECOMMENDED DAILY ALLOWANCE (RDA)
- We don’t have enough scientific evidence to set an official RDA requirement for manganese. Therefore, the Food and Nutrition Board at the Institute of Medicine set an adequate intake (AI) value.
- An adult woman needs about 1.8 milligrams per day, and an adult man needs about 2.3 milligrams per day.
BEST FOOD SOURCES
- The best sources of manganese are plant foods, with a special emphasis on spices. A Paleo diet rich in plant foods and spices will provide adequate manganese.
- Carnivore diets may be low in manganese because those who don’t eat enough veggies or don’t like their veggies can have a difficult time getting adequate manganese. But if they focus on getting adequate spices such as cloves, ginger, saffron, cardamom, cinnamon, and turmeric, then they may very well get adequate manganese.
- Here are some examples of foods that are high in manganese:
- Mussels are the only animal food that is high in manganese.
- Other options include nuts and seeds, grains, legumes, and then fruit categories that include pineapples, coconut, grapes, and berries.
- And then specific vegetables including potato skins, kale, seaweed, spinach, okra, collard greens, and stinging nettles.
- I do want to remind you, related to nuts and seeds and grains and legumes, they need to be properly prepared, such as soaking and sprouting to help release the manganese that can get bound to phytic acid in that food so it’s available for the body to use.
NOTES
- Based on scientific studies, iron and manganese may compete for common absorption and transport pathways. Iron supplementation may cause lower manganese absorption and result in decreased MnSOD activity. This was based on one study. Then during iron deficiency, manganese intestinal absorption is increased and resulted in higher levels of accumulation in the brain, which could be problematic.
- Supplementing with manganese and calcium together may slightly decrease manganese bioavailability because the calcium might outcompete it.
Molybdenum
FUNCTION
- Molybdenum has four primary roles in the human body.
- Reduces sulfites, a toxic form of sulfur, to sulfate, which the body can then either use or excrete in the urine. We get sulfite from eating foods high in sulfur compounds, like meat, eggs, dairy, beans, onions, garlic; cruciferous vegetables like broccoli and cauliflower; supplements like glutathione, taurine, and NAC; certain medications; and some can even be made from gut bacteria. Pregnancy might also increase our sulfite levels.
- Converts purines to uric acid. Examples of purine-rich foods are organ meats, meat, fish and seafood, beer, asparagus, cauliflower, spinach, and mushrooms. The building blocks of DNA and RNA are also purines. Uric acid is a beneficial antioxidant that is protective in our body as long as it does not get too high. Uric acid that is too high can result in a form of arthritis called gout. You can see that molybdenum is important for our DNA, RNA, as an antioxidant, and also could be a player in gout.
- Molybdenum can help detoxify drugs, including nicotine and other toxins.
- It provides protection against DNA damage.
DEFICIENCY/TOXICITY
- Symptoms of sulfite sensitivity, such as insomnia, mood disorders, poor motivation, low ability to cope with stress, chronic pain, fatigue and morning sickness might result if there’s not enough molybdenum. Also think of symptoms associated with vitamin B1 or vitamin B6 deficiency.
- Taking a supplement with sulfate in the name such as magnesium sulfite, or sulfate, should be taken away from high molybdenum food so it doesn’t interfere with the absorption of molybdenum.
- Oversupplementing with molybdenum can raise uric acid levels in some people and trigger gout and pretty severe joint pain.
- Molybdenum also may contribute to copper deficiency. When molybdenum binds to sulfate, it’s then able to bind to copper and pull it out of the body and excrete it.
RECOMMENDED DAILY ALLOWANCE (RDA)
- On average, about 45 micrograms per day for adults. The recommendations are based on one small study of four young men and then adjusted mathematically for the other categories above.
- A clinician might make adjustments to the above numbers of recommendations based on symptoms of possible sulfite sensitivity symptoms or other possible signs of deficiency and suggest a supplement. Keep in mind that with many nutrients, overfarming our soil may also lead to lower levels in our food supply.
BEST FOOD SOURCES
- Liver, oats, beans (white, lima, red, black-eyed peas, pinto), string beans, peas (yellow split, green), rice.
- Foods with lower levels of molybdenum include asparagus, cottage cheese, eggs, bananas, spinach, potatoes, cabbage, squash, tomatoes, bean sprouts, cantaloupe, nuts, chicken, and milk.
NOTES
- Diets that are higher in sulfur-containing foods will use up more molybdenum to process the extra sulfur. These foods are animal proteins, onions, garlic, and cruciferous vegetables. Eating more of these foods might increase normal requirements of molybdenum for people following a Paleo diet. Eating liver weekly as a good source of molybdenum will help ensure adequate molybdenum.
Niacin (B3)
FUNCTION
- Acts as an electron carrier in the body, playing crucial roles in carbohydrate, fatty acid, and protein metabolism.
- Is required for the synthesis of ribose, which forms part of the sugar backbone of DNA.
- Involved in DNA repair and is therefore crucial for genome stability.
- May play a role in cancer prevention.
- Part of the mobilization of calcium. Calcium signaling is involved in critical processes such as neurotransmission, insulin release, and muscle contraction.
BEST FOOD SOURCES
Chicken breast, salmon, ground beef, liver, roasted peanuts, avocado, mushrooms, sunflower seeds, potato, coffee, milk or cheese
RECOMMENDED DAILY ALLOWANCE (RDA)
- No extensive storage
- Can be synthesized from the amino acid tryptophan, the requirements from the Institute of Medicine are given as dietary niacin equivalents.
- One niacin equivalent is equal to 1 mg of niacin or 60 mg of tryptophan.
- Adult men require 16 niacin equivalents per day
- Adult women need 14 niacin equivalents per day
NOTES
- Since niacin can also be synthesized from tryptophan by a process requiring iron and vitamin B6, symptoms of niacin deficiency will only occur with deficiency of niacin itself and either deficiency of protein, iron, or vitamin B6.
- Niacin toxicity can cause what is called niacin flush, where the body’s capillaries are excessively dilated. This may be painful and accompanied by a rash, hives, sweating, and blurred vision. Niacin toxicity can also cause liver damage and impaired glucose tolerance. The upper limit set by the Institute of Medicine is 35 niacin equivalents per day for adults, so toxicity is rare unless an individual is supplementing with large doses of nicotinic acid.
- There is no extensive storage of niacin in the body, so we require daily intake. Niacin can be synthesized from tryptophan, as I said before. However, it takes an estimated 60 mg of tryptophan to produce 1 mg of niacin, and serotonin production also competes for tryptophan.
- In most cases, consuming adequate niacin-rich foods and correcting deficiencies in iron, protein, or vitamin B6 should correct a niacin deficiency. However, some people may benefit from niacin supplementation, particularly if they are in a high-risk category for deficiency.
- High doses of niacin have been shown to improve lipid profiles in those not taking statins, though they do not reduce the number of cardiovascular events. If it is within your scope of practice to recommend supplements, Chris recommends the nicotinamide riboside form of niacin, as these supplements are much less likely to cause niacin flush. However, high doses can still overload the body’s methylation systems, so methylation status should be monitored by a healthcare practitioner if supplementing with niacin.
Pantothenic Acid (B5)
FUNCTION
- It is the functional moiety of coenzyme A, also known as CoA.
- Carbohydrates, protein, and fat are all broken down to acetyl-CoA.
- Acetyl-CoA can then be used for ketone synthesis, fatty acid synthesis, steroid synthesis, or it can enter the TCA cycle and be oxidized to provide cellular energy.
- Without CoA, all metabolism suffers.
BEST FOOD SOURCES
Pantothenic acid gets its name from the Greek pantos for “everywhere” because pantothenic acid is found in a wide variety of food sources.
Beef liver, shitake mushrooms, sunflower seeds, avocado, chicken breast, russet potatoes, eggs, ground beef, broccoli
RECOMMENDED DAILY ALLOWANCE (RDA)
- Since evidence in humans for pantothenic acid requirements is limited, the Institute of Medicine has established adequate intake values as opposed to RDAs.
- Adults are estimated to require 5 mg per day.
NOTES
- Pantothenic acid deficiency is rare since the body conserves pantothenic acid as CoA.
- Symptoms of deficiency include vomiting, nausea, stomach cramps, insomnia, and fatigue.
- Too little pantothenic acid can also cause depression, irritability, numbness of the hands and feet, restlessness, and apathy.
- Some individuals may also experience low blood sugar and increased sensitivity to insulin.
- Risk factors for deficiency include a diet high in refined grains and devoid of pantothenic acid-rich foods.
- Gut dysbiosis may also contribute to pantothenic acid deficiency.
- There are no reported toxicities of pantothenic acid.
- The gut microbiota synthesizes some vitamin B5, though the amount it contributes to overall vitamin B5 status is unknown.
- Pantothenic acid can be destroyed by excessive freezing, canning, and refining but is plentiful in whole foods.
- Any treatment protocol for remediating vitamin B5 deficiency should primarily be focused on consuming pantothenic acid-rich foods.
- Jarrow Formulas Pantethine.
- Many B complexes also contain pantothenic acid.
Phosphorus
FUNCTION
- Phosphorus is a macromineral.
- It is a component of the structural phospholipid bilayer of our cell walls. Bilayer cells means each wall has a top and bottom layer that’s made up of about 10 percent phosphorus.
- It is also part of the structure of our DNA and RNA, or the nucleotides. Our DNA is about 30 percent phosphorus.
- Phosphorus assists with protein regulation and energy production from sugar and lipids via phosphorylation. Phosphorylation is the attachment of a phosphoryl group, which is a combination of phosphorus and oxygen. An example is when the body converts a glucose molecule to pyruvate, making ATP, another name for energy in the human body. This process is called glycolysis.
- Phosphorus helps maintain normal acid–base balance as one of the most important buffers in the human body. Here’s an example. Changes in acid–base balance affect phosphate and calcium. In early renal failure, phosphate excretion decreases due to decreased glomerular filtration rate in the kidneys. The kidneys are not able to do their job very well. Increased phosphate in the blood binds to calcium, producing hypocalcemia in the blood. The body senses the low calcium and pulls from the bone stores. This could end up resulting in osteoporosis.
- Phosphorus also assists with bone mineralization.
DEFICIENCY/TOXICITY
Phosphorus deficiency is very rare, but it can occur in certain circumstances:
- Rickets in children
- Osteomalacia in adults
- Low vitamin D and calcium
- Refeeding Syndrome: starvation and eating disorders over extended period of time
- People at risk for deficiency: alcoholics, diabetics due to renal insufficiency in later stages, some medications such as antacids, fruitarians, people with a very high-fat diet such as Keto.
Phosphorus toxicity:
- Tetany is an acute condition that is due usually to low blood calcium, called hypocalcemia, and is characterized by spasms of the hands and feet, cramps, spasms of the voicebox, or the larynx, and overactive neurological reflexes. If phosphorus is too high acutely, it could cause calcium in blood to drop suddenly before enough can be pulled from bone to balance the blood. This is a very rare occurrence.
- When excess phosphorus is combined with excess calcium and vitamin D, this can cause soft tissue calcifications.
- Weak porous bones due to pulling calcium from bones in order to buffer the high phosphorus.
RECOMMENDED DAILY ALLOWANCE (RDA)
Most people get too much phosphorus. It is found in many more foods and is easy to obtain, and so far less likely to result in deficiency. When consuming a natural diet, deficiency is almost impossible. But remember, it needs to be balanced with other nutrients.
- Adults need about 700 milligrams per day.
- A child between ages one and three needs about 460 milligrams per day.
- As children begin to grow and get a little older and increase their growth rate, such as a child ages four to eight, they need about 500 milligrams per day. And then children and adolescents ages nine to 18 in prime growth spurt time periods need about 1,250 milligrams per day.
- Some people actually need to avoid phosphorus, such as people with later stages of kidney disease, and those people who might be on dialysis.
BEST FOOD SOURCES
Sources of phosphorus occur in high amounts in natural food sources. These are listed in order from greatest concentrations to least.
- Very good sources of phosphorus include dairy, eggs, meat, poultry, fish, legumes, nuts, seeds, vegetables, and grains.
- Low to moderate sources of phosphorus include fruit.
- Phosphorus is also an additive in common processed foods. It’s added in quite high amounts in cola, baking powder, Parmesan or American cheese, baker’s yeast, cocoa powder, vegetable spreads for bread, cold cuts, hot dogs, and sausages.
- Phosphorus is also sometimes added in lower amounts to frozen meat, canned seafood, many cheeses, yogurt, chocolate, beer, and instant coffee. The trouble is, these additives are often unlabeled.
NOTES
- Macrominerals are needed in the human body in large quantities and are also present in larger quantities compared to the trace minerals.
- Phosphorus is the second most abundant mineral in the human body, making up about 25 percent of the total mineral content. Of this, about 85 percent is found in the bones and the teeth.
- Calcium and phosphorus make bone together. Vitamins A, D, and K help send calcium and phosphorus both to the right places, bones and teeth, so they don’t make hard tissue together in soft tissue such as artery plaques or kidney stones.
- The ratio between a high phosphorus and low calcium consumption can lead to lower bone density. The Institute of Medicine states that if calcium consumption does not keep pace with phosphorus consumption, then the bones will be triggered to release calcium from bone at the expense of one’s bone density to balance the phosphorus.
- Phosphorus is more readily found in foods compared to calcium. We need a large amount of calcium and phosphorus for bones and teeth, but only tiny amounts for all the other body functions that are required by these two nutrients.
- Phosphorus, calcium, and vitamin D need to be balanced. The more phosphorus you get, the more calcium and vitamin D you need along with it.
- For people who need calcium but not phosphorus, avoid bone meal. A good option instead, in this case, is calcium citrate, which is low in phosphorus.
- When you get too much phosphorus, your vitamin D levels and needs tend to go up as well.
- A well-balanced Paleo food plan really is not at risk for low phosphorus.
Potassium
FUNCTION
- Potassium is an essential mineral and electrolyte in the body.
- It is the primary positively charged ion in the intracellular space.
- It has a very strong relationship with sodium, the primary positively charged ion in the space outside of cells.
- Sodium–potassium pumps are present in many cells of the body, and together they help maintain an electric potential across the membrane. This electric potential plays a critical role in neurotransmission, muscle cell contraction, and kidney function and is also needed for insulin secretion from pancreatic beta cells.
DEFICIENCY/TOXICITY
- People in the United States consume substantially less potassium than they need. According to the National Health and Nutritional Examination Survey in 2013 and 2014, fewer than 2 percent of adults consume adequate potassium.
- The average daily potassium intake from foods among adults was 3,016 mg for men and 2,320 mg for women. In contrast, it has been suggested that our hunter–gatherer ancestors had potassium intakes as high as 11,000 mg per day.
- Higher potassium intakes are associated with a reduced risk of cardiovascular disease and kidney stones and also increased bone mineral density.
- Even mild potassium deficiency can increase blood pressure and sensitivity to salt, meaning that changes in sodium intake will have a greater effect on blood pressure.
- Consuming adequate potassium is likely much more important than restricting sodium for controlling hypertension in most individuals.
- More severe potassium deficiency can cause constipation, muscle weakness, fatigue, frequent urination, hyperglycemia, muscular paralysis, and cardiac arrhythmias. Because of its effect on muscle contraction, severe potassium deficiency can also cause cardiac failure and death.
- Risk factors for hypokalemia include diarrhea, vomiting, inflammatory bowel disease, the use of diuretics and laxatives, and dialysis treatment.
- Magnesium deficiency can also contribute to potassium deficiency by increasing the excretion of potassium in urine. More than half of individuals with clinical hypokalemia or potassium deficiency also present with magnesium deficiency.
- High amounts of dietary potassium do not pose any health risk in individuals with normal kidney function because excess potassium is filtered by the kidney and excreted in the urine. However, in people with poor potassium excretion due to chronic kidney disease or the use of potassium-sparing diuretics or ACE inhibitors, even low intakes of potassium can cause hyperkalemia. Hyperkalemia, or excess potassium in the blood, often does not present with major symptoms, though severe cases can cause heart palpitations, muscle weakness, paralysis, and a pin-like sensation in the hands and feet.
RECOMMENDED DAILY ALLOWANCE (RDA)
Adults require 4,700 mg per day.
BEST FOOD SOURCES
Potassium is found in a wide variety of plant and animal foods.
- Many fruits and vegetables are excellent sources, including potatoes, sweet potatoes, plantains, squash, mushrooms, tomatoes, and bananas.
- Certain types of fish such as halibut and salmon also contain potassium.
- The body absorbs about 85 to 90 percent of dietary potassium.
- It is important to note that many of the plant sources of potassium are also higher in carbohydrates, so those on low-carb diets should pay particular attention to potassium intake and select foods wisely.
- Potassium supplementation is rarely necessary and can lead to dangerous mineral imbalances, so it should only be performed with the consent of a doctor who can closely monitor electrolytes. Potassium supplements should also never be used by anyone with impaired kidney function, diabetes, insulin resistance, or those who are using NSAIDs, ACE inhibitors, or beta-blockers.

Pyridoxine (B6)
FUNCTION
- Vitamin B6 is a generic name for six different compounds with vitamin B6 activity. One of these, pyridoxal 5′-phosphate, or P5P, is the active coenzyme form of vitamin B6.
- In its coenzyme form, vitamin B6 is involved in over 100 enzymatic reactions, including many related to carbohydrate, amino acid, and fatty acid metabolism.
- It is also necessary for the conversion of tryptophan to niacin or serotonin and the conversion of the excitatory neurotransmitter glutamate to the inhibitory neurotransmitter GABA.
- It supports methylation and plays a crucial role in the formation of heme, the protein that carries oxygen in red blood cells.
BEST FOOD SOURCES
Beef liver, fish, other meats, potatoes and other starchy vegetables, and noncitrus fruit such as bananas.
RECOMMENDED DAILY ALLOWANCE (RDA)
- The body needs a regular supply of dietary vitamin B6.
- Adults require 1.3 mg per day.
NOTES
- Vitamin B6 is fairly resistant to heat degradation, so cooking these foods is not an issue.
- Deficiency is uncommon in young children, but approximately 15 percent of adults and 18 percent of teenage girls are deficient in vitamin B6.
- Signs of severe vitamin B6 deficiency include reduced cognitive function, depression, and confusion. Other signs include scaly dermatitis and microcytic, or small cell, anemia due to a lack of heme protein.
- More moderate vitamin B6 deficiency can cause elevations of homocysteine and contribute to cardiovascular risk.
- Anxiety, insomnia, hypoglycemia, and morning sickness during pregnancy are also possible signs of poor vitamin B6 status.
- Risk factors for poor vitamin B6 status include alcoholism, inflammation, use of oral contraceptives or nonsteroidal anti-inflammatory drugs, and high estrogen levels.
- Vitamin B6 toxicity has a similar symptom profile. It can also lead to depression, fatigue, irritability, and headaches.
- Excess vitamin B6 can also cause skin lesions, convulsions, and nerve damage causing numbness and muscle weakness.
- The tolerable upper limit for vitamin B6 set by the Institute of Medicine is 100 mg per day for adults, so toxicity can only be achieved through chronic high-dose supplementation.
- Achieving higher levels of vitamin B6 through supplementation may be advantageous in some circumstances.
- For example, vitamin B6 has been shown to help with age-associated cognitive decline.
- It also reduces symptom burden in women with PMS.
- Vitamin B6 may also be helpful in reducing morning sickness during pregnancy and in those with dermatitis.
- The ideal supplement form is pyridoxal 5′-phosphate because it does not require activation in the liver, and 5 to 20 mg per day is typically adequate to correct deficiencies that stem from poor dietary intake. Higher doses should only be used in special circumstances under medical supervision.
Riboflavin (B2)
FUNCTION
- Serves as a coenzyme in the body.
- Is essential for proper cellular function, growth, and development.
- A major structural component of proteins in the electron transport chain which is responsible for most of the energy production in cells.
- Helps maintain normal levels of homocysteine.
BEST FOOD SOURCES
Beef liver, yogurt, milk, clams, eggs, beef steak, mushrooms, Swiss cheese, almonds, broccoli, banana
RECOMMENDED DAILY ALLOWANCE (RDA)
Human requires a regular supply of dietary riboflavin. Adult men require 1.3 mg per day, while adult women need 1.1 mg per day.
NOTES
- The conversion of tryptophan to niacin and the activation of vitamin B6 also require riboflavin.
- Riboflavin deficiency is very rare in young children but affects about 2 percent of adults and 5 percent of teens.
- It is uncommon for riboflavin to be deficient without also being deficient in the other B vitamins such as thiamine, niacin, B6, folate, and B12.
- The primary symptoms of deficiency include greasy, scaly dermatitis; lesions on the outside of the lips or corners of the mouth; or inflammation and redness of the tongue. People may also experience fatigue or hair loss.
- Riboflavin deficiency can also cause numbness, pain, weakness, or tingling in the hands and feet (peripheral neuropathy).
- There are no reported toxicities of riboflavin. However, excess riboflavin may turn your urine neon yellow.
- Risk factors for riboflavin deficiency include diabetes, stress, trauma, and the use of oral contraceptives. Vegetarian and vegan athletes may also be at increased risk.
- Bacteria in the large intestine can also produce some riboflavin, and more riboflavin is produced by gut microbes after ingestion of vegetables than meats.
- Riboflavin can be used quite safely either on its own or as part of a B complex if other vitamin B deficiencies are present. Riboflavin supplementation has been shown to be effective in preventing migraine headaches and may be helpful in cases of hypothyroidism and HPA axis dysregulation.
Selenium
FUNCTION
- Selenium is an essential trace mineral that is important for many processes in the body.
- The functional action of selenium is as a component of selenoproteins. Selenoproteins play crucial roles in reproduction, DNA synthesis, and protection against infection and oxidative damage. They help regenerate glutathione, the body’s master antioxidant. Selenoproteins are also responsible for the conversion of T4 to the active T3 thyroid hormone. Studies suggest that selenium may also play a role in the prevention of cancer and cardiovascular disease.
RECOMMENDED DAILY ALLOWANCE
- Selenium does have some storage in skeletal muscle, but we still want to make sure we are getting regular dietary selenium.
- Adult men and women require 55 mcg per day.
DEFICIENCY/TOXICITY
- Overt selenium deficiency is fairly uncommon, only occurring in about 1 percent of adults and 2 percent of teens.
- Moderate selenium deficiency can increase vulnerability to environmental toxins and infections. It may also reduce conversion of the inactive T4 to active T3 thyroid hormone.
- Severe selenium deficiency can cause Keshan disease, which primarily affects children and younger women and causes death of muscle heart tissue and chronic liver damage.
- Risk factors for selenium deficiency include living in selenium-deficient regions, chronic kidney disease requiring hemodialysis treatment, and HIV-positive status.
- Selenium concentrations also tend to decline with age.
- Selenium can also be toxic when chronically consumed or supplemented in excess. The toxicity syndrome is called selenosis and is characterized by garlic breath odor, nausea, weakness, diarrhea, hair and nail loss or brittleness, skin rashes, fatigue, irritability, and nervous system disorders.
- Acute toxicity can also cause gastrointestinal symptoms, acute respiratory distress, muscle tenderness, kidney failure, and, in rare cases, death.
- Moderate toxicity of selenium may increase diabetes risk.
- The tolerable upper intake level set by the Institute of Medicine is 400 mcg per day for adults.
- Dietary absorption of selenium is very efficient, with 84 to 98 percent of selenium being absorbed.
BEST FOOD SOURCES
- The selenium content in plants varies widely by geographical location and is dependent on the amount of selenium in the soil. The Midwest, East Coast, and Northwest Coast of the United States have particularly low selenium levels in the soil, but even within a state or county, there is enormous variability in soil selenium content. Soil depletion of selenium has a much greater impact on selenium levels in plant products than in animal products.
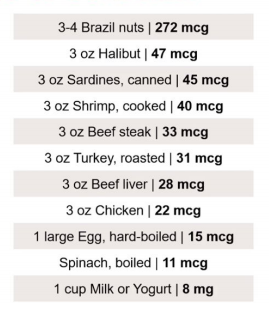
- Brazil nuts are an incredibly selenium-rich food. Just three to four nuts provides well over the daily requirement for selenium.
- Besides Brazil nuts, seafoods and organ meats are the richest dietary sources of selenium. Muscle meats, eggs, and dairy also provide some dietary selenium.
- If consumption of Brazil nuts, seafood, and organ meats does not correct deficiency, supplementation of selenium can be considered.
- Selenium is a micronutrient with a very tight U-shaped curve, meaning it is very easy to get too little or too much, so extreme care should be taken when supplementing to monitor nutrient status.
- Supplementing with selenium in the context of low iodine status may actually aggravate hypothyroidism, so it is important to keep the synergy of these nutrients in mind.
- I suggest 100 mcg per day of the selenomethionine form.
Sodium
FUNCTION
- Sodium, or salt, is an essential micronutrient.
- It is the primary cation, or positively charged ion, in the fluids that surround the cells and is crucial for maintaining blood volume and proper cardiovascular function.
- Sodium is also crucial for nerve transmission and mechanical movement.
- Over-restriction of salt can be harmful to our health.
RECOMMENDED DAILY ALLOWANCE (RDA)
- According to the Institute of Medicine, adults require 1,500 mg of sodium per day. This value is based on replenishment of sodium lost daily through sweat and urination.
- The actual physiological requirement of sodium to sustain life is only about 500 mg per day.
DEFICIENCY/TOXICITY
- True sodium deficiency can result in low blood levels of sodium, a condition called hyponatremia.
- Symptoms of hyponatremia include brain swelling, coma, congestive heart failure, cardiovascular collapse following acute blood loss, and impaired cardiovascular response to stress.
- Mild sodium insufficiency stimulates the renin–angiotensin–aldosterone hormone system, which regulates blood pressure and blood volume.
- A low-salt diet may also increase blood cholesterol and triglycerides, increase the risk of stroke and heart attack, and shorten lifespan.
- Sodium is also required for the intestinal absorption of many nutrients, so a lack of sodium may result in deficiencies in vitamin C, biotin, phosphorus, magnesium, iodine, and vitamin B5.
- Risk factors for sodium deficiency include intense endurance athletics, chronic stress, food-borne illness, gastrointestinal infections, diabetes, use of diuretics, and the use of saunas.
- The Institute of Medicine has suggested a tolerable upper limit of 2,300 mg per day, or about 1 teaspoon of salt. The USDA dietary guidelines urge Americans to consume less than 2,300 mg of sodium per day, while the American Heart Association has an even more strict guideline, recommending less than 1,500 mg per day for general health and disease prevention.
- To provide some context, the average intake of sodium for American adults is about 3,300 mg of sodium per day, which is well above the standard recommendations.
- Excessive amounts of sodium can cause problems, especially in the context of low potassium.
- High sodium-to-potassium ratio can increase blood pressure and increase the volume of the fluid surrounding cells, resulting in swelling or edema. It may also disrupt acid–base balance, lowering bone mineral density and increasing the risk of osteoporosis and kidney stones.
- If the serum concentration of sodium rises, this is called hypernatremia. It usually results from inadequate water intake, not excess salt intake, and requires immediate medical treatment. Early symptoms of hypernatremia include inability to sense thirst, nausea, weakness, and loss of appetite. Untreated hypernatremia can lead to cerebral edema, confusion, seizures, muscle spasms, coma, and death.
- Blood levels of sodium are tightly regulated by the kidneys, which determine how much sodium and water is excreted in the urine. Aldosterone, a steroid hormone secreted by the adrenal glands, helps regulate the balance of sodium and water in the body. An abrupt increase in dietary salt can cause a transient redistribution of fluid from the inside to the outside of cells, but after a few days, the kidneys are usually able to compensate with excess sodium excretion to match dietary intake. Therefore, healthy people are generally able to adapt to a wide range of salt intakes without a significant change in blood pressure or other health parameters. This is especially true if they are consuming adequate potassium.
- There are a few health conditions in which lower salt consumption may be necessary. First, there is evidence that some hypertensive individuals have inherited salt sensitivity, caused primarily by impaired sodium transport into the kidney. People with this trait will have a significant blood pressure response to high salt intake. However, increasing potassium in these individuals suppresses salt sensitivity in a dose-dependent fashion. Consuming adequate potassium, therefore, may be far more important for treating high blood pressure than restricting salt.
- Though evidence is mixed, patients with chronic renal disease may also have better outcomes consuming a lower amount of salt.
- Those who are at high risk of kidney stones or osteoporosis may need to reduce salt intake, as high sodium excretion also leads to a higher level of calcium excretion in the urine. While salt recommendations will vary between individuals based on age, gender, physical activity, and health conditions, overall, the data support an intake between 3,000 and 7,000 mg of sodium, or 1.5 to 3.5 teaspoons of salt per day. People who are quite active or sweat a lot should consume salt on the higher end of this spectrum, and those who are less active may want to consume on the lower end.
- For the majority of healthy individuals, avoiding processed foods and salting to taste will provide an appropriate level of sodium in the diet.
BEST FOOD SOURCES
- Natural sources of sodium include sea vegetables, fish, shellfish, and meat plus certain plants such as beets, carrots, celery, spinach, and turnips.
Thiamin (B1)
FUNCTION
- Crucial for carbohydrate metabolism, including the conversion of pyruvate to acetyl-CoA which is important for the production of the neurotransmitter acetylcholine and the production of myelin.
- Important for the metabolism of certain fatty acids and the synthesis of nucleic acids.
BEST FOOD SOURCES
Pork chops, trout, mussels, acorn squash, watermelon, ground beef, yogurt, potato, orange
RECOMMENDED DAILY ALLOWANCE (RDA)
- No extensive storage
- According to the Institute of Medicine, adult men require 1.2 mg per day, while adult women require 1.1 mg per day.
NOTES
- Thiamin deficiency can lead up to the buildup of pyruvate, causing acidosis.
- Mild thiamin deficiency can disrupt circadian rhythms and contribute to HPA axis dysregulation.
- Other symptoms of deficiency include muscular weakness, an enlarged heart and possible cardiac failure, anorexia, weight loss, apathy, poor short-term memory, confusion, and irritability.
- Severe deficiency can result in several diseases including beriberi, Wernicke’s encephalopathy, and Korsakoff psychosis. These conditions require emergency medical treatment to prevent seizures, paralysis, and death.
- Risk factors for thiamin deficiency include malabsorption disorders, bulimia, liver disease, chronic alcoholism, and a diet low in animal products and high in unenriched processed foods. The elderly and people with diabetes are also at increased risk.
- Several genetic inborn errors of metabolism can also cause symptoms of thiamin deficiency. Improved newborn screening can typically catch children with these abnormalities early.
Vitamin A
FUNCTION
- Vitamin A is actually a group of fat-soluble compounds called retinoids, which include retinol, retinoic acid, and retinyl esters.
- It is critical for vision. It is a component of rhodopsin, which is the protein that absorbs light in the retina.
- It is required for the assimilation of protein, minerals, and water-soluble vitamins. It supports cell growth and differentiation. It acts as an antioxidant, and it plays a crucial role in reproduction and promotes full-term pregnancy along with proper development of the fetus, particularly the facial structure.
- Two forms of vitamin A:
- Preformed or active vitamin A: retinol and retinyl esters. This is found almost exclusively in animal foods, particularly liver and egg yolks.
- Then there are vitamin A precursors such as beta-carotene and other carotenoids, and these are found primarily in vegetables and fruits. All forms of vitamin A require fat for absorption, even the carotenoids.
- Carotenoids must be converted into retinol, or retinoic acid, the active form of vitamin A, in order to be utilized in the body, and this conversion is extremely inefficient. You must eat 19 to 48 times as much beta-carotene to obtain the same amount of active vitamin A, or retinol. Beta-carotene consumption does not increase serum levels of retinol, even when levels are low to begin with. Some evidence shows that up to 50 percent of the population has a genetic profile that prevents the body from converting enough carotenoids into active vitamin A. These people must consume animal sources of vitamin A to avoid deficiency, but most Americans no longer consume foods that are rich in preformed active vitamin A.
RECOMMENDED DAILY ALLOWANCE (RDA)
- The recommendations for vitamin A are measured in retinol activity equivalents, or RAE, to reflect the different bioavailability of plant versus animal forms of vitamin A.
- One microgram of retinol equals about 19 to 48 mcg of carotenoids, so again, you have to eat 19 to 48 times as many carotenoids to get 1 mcg of retinol.
- The RDA for vitamin A is 900 RAE for adult men, 700 for adult women, 750 to 770 for pregnant women, and then 1,200 to 1,300 for lactating women. The average intake for Americans two years and older is only at 607 RAE, so that is too low.
- Anthropological evidence shows that our ancestors ate much, much larger amounts of vitamin A than even the most progressive modern recommendations. For example, the traditional Inuit consumed as much as 10,500 RAE daily. Frank deficiency of vitamin A is rare in the United States, since vitamin A is stored in the liver in the form of retinyl esters.
DEFICIENCY/TOXICITY
- Deficiency is more common in third-world countries. Long-term, severe deficiency can lead to blindness, chronic diarrhea, and mortality from infection.
- Symptoms of suboptimal vitamin A status include poor vision at night, keratosis pilaris—this is the chicken skin that can happen on the back of arms, particularly the back of the upper arm—dry skin, dry eyes, frequent infections, acne, eczema, psoriasis, menstrual dysfunction, hypothyroidism, autoimmune disease, and infertility or difficulty conceiving. Deficiency in animals can cause impaired steroid hormone synthesis, so problems with producing cortisol, DHEA, and other hormones. A link has been established between vitamin A deficiency and autoimmune disease. Vitamin A may help balance immune function along with vitamin D in those situations. Vitamin A can help calm down an overactive immune system.
- There have been a lot of concerns about the toxicity of vitamin A expressed, but is vitamin A really toxic at levels that are typically consumed? As I mentioned, vitamin A is fat soluble and is stored in the liver, so levels can accumulate over time. An excessive intake of preformed vitamin A can lead to toxicity. The symptoms of toxicity include headaches, dizziness, nausea, skin irritation, bone and joint pain, liver abnormalities, coma, and possible death, although that is almost unheard of. It could potentially cause birth defects in extremely large doses during pregnancy, but that would most likely be from excessive supplementation or pharmaceutical retinoids, not dietary intake or even typical levels of supplementation. However, taking vitamin A together with vitamins D and K2 significantly reduces the risk of toxicity and raises the threshold at which vitamin A causes toxicity. In other words, if you take vitamins D and K2, you are going to greatly increase the amount of vitamin A you can take without problems. One study showed that the dose necessary for toxicity symptoms from vitamin A increased by an extra 175,000 IU per day when paired with vitamin D, so that is the amount in five tablespoons of cod liver oil—a huge amount of vitamin A that would far exceed what most people would take in supplemental forms. Most toxicity symptoms of vitamin A are associated with elevated blood calcium, which could be affected by vitamin K2 supplementation because vitamin K2 removes calcium from the blood and puts it in the hard tissues such as the bone and the teeth where it is needed. In theory, taking vitamin K2 would help mitigate that potential side effect of excess vitamin A.
- Supplementation with beta-carotene does not cause acute toxicity, but it is associated with increased risk of lung cancer and cardiovascular disease, which is another reason to focus on getting preformed vitamin A instead of the precursors such as beta-carotene. Pregnant and breastfeeding women need more vitamin A, not less, and unfortunately, they have been scared away from taking vitamin A supplements such as cod liver oil because of this concern about vitamin A toxicity, which can easily be addressed by making sure that your vitamin D and vitamin K2 levels are adequate.
BEST FOOD SOURCES
- The best source of vitamin A in the diet by far is liver, whether it comes from beef, lamb, chicken, goose, turkey, or fish. Four ounces of beef liver, for example, contains about 18,000 to 20,000 IU of vitamin A. Consuming four to eight ounces of liver per week would provide adequate vitamin A for most people, even assuming no other intake of vitamin A in the diet.
- People with iron storage disorders or copper overload should not consume liver because it is very high in those nutrients as well.
- Be aware that many clients with histamine intolerance also are not able to consume liver.
- Fish liver, like cod liver, is another great source of vitamin A, and this is usually consumed in the form of cod liver oil. This has been consumed in Scandinavia and other parts of northern Europe regularly as part of the diet for many, many generations, and I think it is probably the easiest way for people to get vitamin A in their diet, especially if they do not enjoy consuming liver and other organ meats.
-
- I like the extra-virgin cod liver oil from Rosita Real Foods. It is my favorite and the one that we use at home, but there are many good options out there now. 10,000 to 15,000 IU per day of vitamin A is a safe daily amount for adults. Again, I think it is best to get it from a food source such as liver or cod liver oil. Pregnant and breastfeeding women with good vitamin D status should tolerate 10,000 to 15,000 IU per day easily and could go much higher than that. They could easily double that provided they are consuming adequate vitamin D and vitamin K2 in their diet. Again, supplements, if they are not taking cod liver oil, which is fat, if you are taking a retinol supplement or a supplement with retinol in it, it should be taken with a fat-containing meal for optimal absorption.
- Eggs from pasture-raised chicken are also a really good source of vitamin A. They are not anywhere near as high in vitamin A as liver is, but they still can be a good source. One pastured egg yolk is about 800 IU of vitamin A. This can be a really great source of vitamin A for children and babies. Note that conventionally raised eggs will not have vitamin A levels this high.
- Orange and yellow vegetables are a good source of beta-carotene, which is a vitamin A precursor. Some beta-carotene, as we have discussed, is converted into active vitamin A in the body. Carotenoids from foods are potent antioxidants, so they have other benefits above and beyond being vitamin A precursors. Food sources would include things such as sweet potato, bell pepper, spinach, carrots, cantaloupe, mango, apricots, broccoli, pumpkin, and squash. As I mentioned before, consuming fat with these vegetables and fruits will significantly increase the bioavailability of beta-carotene.
Vitamin C
FUNCTION
- Vitamin C cannot be made by humans, unlike most other mammals. We have to get it from the diet.
- It is an antioxidant, a cofactor for many enzymatic reactions, for example, helping to produce collagen and neurotransmitters.
- It also helps to maintain proper levels of glutathione.
RECOMMENDED DAILY ALLOWANCE (RDA)
- The RDA for vitamin C is 90 mg per day for men and 75 mg per day for women.
- You could add 35 mg per day for smokers, since they are under oxidative stress.
DEFICIENCY/TOXICITY
- Insufficient intake of vitamin C is common. Thirty-four percent of men and 27 percent of women do not get enough of it from the diet. Low intake is even more common in the elderly and those struggling with chronic disease.
- The vitamin C level for optimal level is higher than the RDA. I would recommend at least 150 mg per day or higher amounts for those dealing with chronic diseases that involve oxidative stress and inflammation.
- Symptoms of insufficient intake can vary, but the most common symptoms of deficiency are poor wound healing and fatigue. These symptoms are due to the role of vitamin C in collagen production and neurotransmitter production.
- Higher vitamin C intake has a lot of proven benefits. There is an inverse association between vitamin C intake and cardiovascular risk, meaning higher intake confers lower risk. Plasma vitamin C concentrations are also inversely associated with hypertension and with gout.
- There is a strong inverse association finally between blood levels of vitamin C and death from all causes. Every 20 mmol/L increase in plasma ascorbic acid levels (vitamin C) is associated with about a 20 percent risk reduction in death from all causes.
- Those who need higher vitamin C intake include all of the conditions I just mentioned as well as women on estrogen-containing birth control or those who regularly use aspirin.
- Be cautious of large doses of vitamin C for people who are taking anticoagulant drugs. The evidence is controversial, but some studies suggest that vitamin C may block the action of these drugs.
BEST FOOD SOURCES
- Food sources of vitamin C are fortunately plentiful.
- Red peppers have 95 mg per half cup.
- One orange has about 70 mg.
- A medium kiwi has 64 mg.
- A half cup of cooked broccoli has 51 mg.
- One cup of fresh strawberries has 49 mg.
- Half a grapefruit has 38 mg.
- Aim for about 150 mg per day.
- Combining vitamin C with iron-containing foods will increase the absorption of iron. This can be useful if you are anemic due to iron deficiency, and we will often recommend that those patients take vitamin C with their food, especially the high iron-containing meals. But the opposite can also be true. If you have hemochromatosis, a condition characterized by excess iron levels, then you would want to avoid taking vitamin C around iron-rich foods.
- If you have chronic illness or you would like to prevent some of the conditions I mentioned earlier that benefit from increased vitamin C intake, you could aim for as much as 500 mg to 1,000 mg per day or more. This would usually be achieved by adding a vitamin C supplement. The upper limit for vitamin C is set at 2,000 mg per day, or 2 g per day, although this is mostly due to loose stool and abdominal discomfort that can arise from taking vitamin C. There is not any evidence that I am aware of regarding toxicity of vitamin C, even at very high doses up to 5 g per day. Oral liposomal form of vitamin C often allows a much higher dose to be consumed without the digestive side effects, but even if you are taking a liposomal form, and certainly with other forms of vitamin C, it is best to spread out doses throughout the day to reduce the likelihood of digestive discomfort and also not to pair vitamin C with high doses of magnesium, which can also have a laxative effect.
- Here are some examples where using supplemental vitamin C can be beneficial. Vitamin C supplementation reduces blood pressure in both people with normal blood pressure and people with hypertension. Vitamin C is used by some integrative clinicians in cancer treatment. It can be used to reduce exercise-induced asthma, and it can be useful in HPA axis dysregulation, given that the adrenals have a very high concentration of vitamin C, and vitamin C is used up quickly in states of high stress.
Vitamin D
FUNCTION
- Vitamin D is actually a vitamin-like hormone that is largely produced in the skin when it is exposed to ultraviolet radiation.
- The active form of vitamin D is called calcitriol, or 1,25(OH)D, and it is converted from vitamin D2 in the kidneys in small amounts.
- The most common lab-tested form of vitamin D is D2, or 25(OH)D, which is also called calcifediol. It is a pre-hormone. It is not the active form, but it is considered to be a good marker of vitamin D status.
- The best-known role of vitamin D is increasing the intestinal absorption of calcium. It helps maintain calcium and phosphate levels in the blood, and it enables the proper mineralization of bone. It also protects against osteoporosis, rickets, and fracture, and it plays a number of other important roles in the body.
DEFICIENCY/TOXICITY
- Vitamin D deficiency has also been linked to increased risk of heart attack, cancer, severe asthma, autoimmune disease, type 2 diabetes, and death from all causes.
- With vitamin D, balance is key. Research suggests that too much may be a problem, and most people are, unfortunately, not aware of this. There is little evidence that raising levels above 50 ng/mL is beneficial, and there is some evidence that it may be harmful in some cases. Higher vitamin D levels, certainly in the toxic range above 100 ng/mL, but even in the upper part of the normal range, such as 80 to 90 ng/mL, have been linked with decreased bone density, heart attack, stroke, and kidney stones.
- The optimal blood level of 25(OH)D is still controversial. An exhaustive review of nearly 1,000 studies by the Institute of Medicine suggested that a range of 25 to 50 ng/mL was ideal. However, vitamin D advocates such as Dr. Michael Holick have suggested a much higher range. Labs such as Quest and LabCorp have adopted this suggestion and use a reference range of 30 to 100 ng/mL. Yet there is almost no evidence that pushing vitamin D above 60 ng/mL has any benefit, and some studies suggest harm. What’s more, randomized control trials investigating the effects of supplementing with vitamin D on many conditions have produced disappointing results. Given the uncertainty, I think the optimal range for most people for 25(OH) vitamin D is between 35 and 60 ng/mL.
- Also, new evidence suggests that there is no one-size-fits-all approach to vitamin D. Some people may require more and some less. Working with a Functional Medicine practitioner who is knowledgeable about vitamin D optimization can be really helpful. Recent evidence suggests that the optimal vitamin D level may vary across populations, and levels that are considered deficient according to conventional reference ranges may actually be sufficient for some people.
- For example, blacks have lower 25(OH)D levels than whites, even in their ancestral latitudes.
- Nonwhites with abundant sun exposure in Hawaii have so-called low vitamin D status, according to the reference range but no indication of biological vitamin D deficiency.
- People with non-white ancestry may be adapted to lower levels of 25(OH)D than people with white ancestry.
- Also, nonwhites may require less parathyroid hormone to activate 25(OH)D in the face of inadequate calcium. The research is still evolving here, but it is clear that we need more individualized assessment of vitamin D status in the future rather than just applying the lab range to everyone without consideration of their ethnic background.
BEST FOOD SOURCES
- Only about 10 percent of vitamin D requirements come from food in the typical diet. The sources are similar to vitamin A, so cod liver and cod liver oil. The cod liver oil supplement can kind of kill two birds with one stone there.
- Cold-water fatty fish in species such as marlin, herring, fatty tuna, rainbow trout, salmon, sardines, and mackerel have about 250 to 1,000 IU of vitamin D per 3.5-ounce serving.
- Egg yolks—again, pastured eggs will contain much more vitamin D than conventional eggs, in this case, about four to six times more. Some reports have suggested that mushrooms may be a good source of vitamin D, but they contain D2, which is the less active form, rather than D3, so I do not think they will make a meaningful contribution to vitamin D levels for most people.
- For vitamin D supplementation, many people will have to do this because they live in a place where sun exposure really is not an option or their job or lifestyle does not permit it, and they cannot get enough from food. Individual response to supplementation varies. Clients should work with a practitioner to test vitamin D levels every three to six months and determine their optimal dosage. Clients should not supplement if blood levels are above 50, in my opinion, except in specific circumstances, or if levels are between maybe 30 and 50 or 25 and 50 and the client gets regular unprotected sun exposure. Recommended supplements: I prefer the cod liver oil because it is a food-based form, if possible. Another option would be vitamin D drops. Sometimes they come with vitamin K2 as well, which is a good combination. You can supplement with 3,000 to 5,000 IU per day if blood levels are below 25. If blood levels are between 25 and 50, some clients will require a maintenance dose of 1,000 to 2,000 IU per day, especially during the winter months.
SUNLIGHT
- Ultraviolet light exposure is really the best option for vitamin D if it is available and possible. Sunlight has been the primary source of vitamin D for humans throughout our history. Most modern humans get very little sun exposure due to indoor work environments, long sleeves and pants covering the skin, living far from the equator, and putting sunscreen on every time right when you step out the door. Stress, inflammation, obesity, and old age will reduce the efficiency of vitamin D production by the skin in response to exposure to ultraviolet light. In general, full-body exposure to the midday summer sun will produce about 10,000 IU of vitamin D in about half the amount of time it takes the skin to turn pink. That could be as little as 15 minutes with someone with pale skin or as long as an hour or more in someone with darker skin. It is important to understand that there are many factors that affect the production of vitamin D from the sun, including skin tone. Pale skin requires far less time than dark skin. If you are at an equatorial latitude, the time will be much shorter than it would be if you were at a far northern or southern latitude. The amount of skin exposed, the time of day and the time of year—both of which affect the solar angle, the angle of the sun in the sky—of course, in summer at noon it is going to be a much shorter period of exposure required for vitamin D than winter at 4 p.m. You can mitigate the risk of skin cancer by avoiding sunburn and then covering up after you have had the adequate amount of sun exposure. There has been a lot of concern expressed about skin cancer and sun exposure, appropriately in some cases, but I think the pendulum has swung too far back in the other direction, and now people are unnecessarily, and unfortunately, harmfully, not exposing themselves to any sun at all without sunscreen. Aiming for getting exposure about half the amount of time it takes your skin to turn pink is a good guideline, about three to five times a week if that is possible. It is something good to shoot for.
Vitamin E
FUNCTION
- This is an example of a crucial nutrient that we all need, but it’s also one of these nutrients that we need to be extra cautious about because too much of it can be pretty problematic.
- It is a potent, fat-soluble anti-inflammatory compound that protects us from free radicals and oxidative stress.
- It is also involved in immune function, cell signaling, regulation of gene expression, and other metabolic processes.
RECOMMENDED DAILY ALLOWANCE (RDA)
- The recommended daily allowance is 15 milligrams per day, and most Americans get that from polyunsaturated industrialized seed oils. But on a healthy, nutrient-dense Paleo-type diet due to the damaged types of fats in those industrialized seed oils.
DEFICIENCY/TOXICITY
- Alpha-tocopherol is the form that most supplements contain. This slide shows an example of one type of vitamin E supplement called tocotrienols.
- While vitamin E is an important nutrient to get in your diet, we do not recommend supplementing with it. At best, alpha-tocopherol shows no benefit. But some studies actually show harm. In fact, a meta-analysis in the Journal of the American Medical Association, with 230,000 total participants, it showed that vitamin E supplementation caused increased risk of death from all causes. A review of 78 randomized controlled trials with almost 300,000 total participants found that vitamin E increased the risk of death by a small but statistically significant margin.
BEST FOOD SOURCES
- It’s best to get vitamin E from whole-food sources. Here are what those are. Nuts and seeds are among the best sources: sunflower seeds, almonds, hazelnuts, and pecans, in particular. Also things such as tomato sauce, avocados, apricot, some fish such as trout, spinach, asparagus, chard, broccoli, and blackberries.
Vitamin K2
FUNCTION
- Vitamin K2 is needed to activate proteins, for example, osteocalcin that regulates calcium metabolism via a process called carboxylation. Carboxylated osteocalcin deposits calcium in the bones and the teeth where it is needed and keeps it away from the soft tissues where it can cause problems, so vitamin K2 can prevent and in some cases even treat osteoporosis or bone loss. It also prevents the calcification of soft tissues such as the lining of the arteries, and this lowers the risk of atherosclerosis and heart attacks. In one study, people with the highest intake of vitamin K2 had a 52 percent lower risk of aortic calcification, 41 percent lower risk of coronary heart disease, 51 percent lower risk of death from heart disease, and 26 percent lower risk of death from all causes. This is a significant effect.
- It reduces the risk of fractures by 81 percent.
- It prevents the calcification of elastin in the skin.
- It is required for the proper function of vitamins D and A. All of the fat-soluble vitamins such as K2, D, and A work together synergistically. Vitamin K2 may prevent the toxicity of vitamins D and A and even prevent some of the deficiency symptoms that can be associated with those nutrients.
- Vitamin K2 reduces the risk of prostate cancer by 35 percent. It may be protective against cancer in general.
- Vitamin K2 supports enzymes in the brain that protect against Alzheimer’s and dementia.
- It may protect against kidney stones.
- It promotes healthy facial bone structure in developing babies.
- It is important to note that vitamin K2 is not the same as vitamin K1.
-
- Vitamin K1 is found in leafy greens such as kale and collards. It is primarily used by the body in blood clotting.
- Calcium regulation is the primary role of vitamin K2.
RECOMMENDED DAILY ALLOWANCE (RDA)
- Research is unclear on how much vitamin K2 is optimal for health.
DEFICIENCY/TOXICITY
- There is no upper limit or toxicity level at this point, and some studies, such as the Japanese osteoporosis studies, have used doses between 30 and 45 mg per day. Vitamin K2 is usually talked about in microgram quantities, so that is an enormously high dose, and not only were there no negative effects, there were really positive changes in people with osteoporosis. There is much more of a risk of deficiency of vitamin K2 than there is in overdosing, and again, vitamin K2 also reduces the likelihood of vitamin A or vitamin D toxicity.
BEST FOOD SOURCES
- Food sources are not very abundant for vitamin K2, unfortunately, and this is probably why most Americans are deficient in vitamin K2, particularly those who are avoiding animal fats and because of the shift to grain-based animal agriculture, since pasture-raised animals are much higher in vitamin K2 than grain-based animals from factory-farming type of conditions.
- Vitamin K2 is mostly found in the fat of animal products and in some fermented soy products.
- Our body is very inefficient at converting vitamin K1 to vitamin K2, and very little is absorbed from bacterial production in our guts.
- The major forms of vitamin K2 in the diet are:
-
- Menaquinone 4, or MK4
-
- MK4 sources include grass-fed, full-fat dairy products such as butter, cream, and cheese. Certain cheeses in particular, such as Gouda and Brie, are very high in vitamin K2. Poultry liver, such as duck liver and chicken liver, but especially goose liver; pastured egg yolks; and pastured organ meats such as pancreas and kidneys would be expected to be high in vitamin K2 but have not yet been measured.
- Menaquinone 7, or MK7
-
- The primary source of MK7 in the diet is fermented food. Natto, which is a fermented soy product that is popular in Japan, is by far the highest source of vitamin K2 in any form, but it has a very strong taste, and many people do not like it. Other fermented foods such as sauerkraut and cheese, as I mentioned, are also really good sources of vitamin K2 and will probably be the primary source of vitamin K2 for most of your clients.
- In terms of supplements, the recommended dose for maintenance supplementation is 100 to 1,000 mcg per day, but again, much higher doses, even in the milligram quantities, have been used in studies for prevention and treatment of osteopenia and osteoporosis, and they appear to be safe and well tolerated. Vitamin K2 is best combined with optimal intake of vitamins A and D. In supplement form, you can take MK7 or MK4. MK7 supplements are natural extracts from natto, the Japanese fermented soy product that I mentioned. It has a longer half-life, so you can take lower doses such as 100 mcg a day. MK4 supplements are synthetic but believed to be chemically identical to the form found in animal fats. They have a shorter half-life, so larger doses are appropriate, such as 1,000 mcg per day or more.
- Some research suggests that MK4 is more effective than MK7 in preventing heart disease and osteoporosis, but both forms are beneficial.
- Another option would be high-vitamin butter oil that naturally contains MK4, but there is no guarantee of dosing when you are using the butter oil, and it may be no better than simply cooking with ghee or adding ghee to foods.
- Supplementation with vitamin K2 may be contraindicated with clients on blood thinners such as Coumadin, or warfarin, and it is better to stick with high-vitamin K2 foods in that case.
Zinc
FUNCTION
- Zinc is an abundant chemical element found in the Earth’s crust and has many industrial applications.
- It is the second most abundant trace mineral in the human body after iron.
- There are about two to four grams of zinc in the human body.
- It is abundant in the brain, muscles, bones, kidney, liver, prostate, and parts of the eye.
- Zinc homeostasis in the human body is controlled by the intestines.
- It functions as a cofactor or catalyst for the function of over 300 enzymes and chemical reactions in the human body.
- It’s key in the proper folding of some proteins. Without zinc, proteins will misfold and result in loss of many functions.
- One example are the metallothioneins. These are metal-binding structures that support some really important functions, including metal ion balance, cellular defense against oxidative stress, detoxification of heavy metals such as mercury, cadmium, and arsenic.
- Zinc supports the unique folding and connections of our DNA for genetic expression.
- It influences hormone release, supports nerve impulse transmission, and apoptosis, which is spontaneous cell death.
RECOMMENDED DAILY ALLOWANCE (RDA)
- Adult males need about 11 milligrams per day and adult females need about 8 milligrams per day.
- Vegetarians and vegans may need higher amounts than is recommended by the RDA.
DEFICIENCY/TOXICITY
- Deficiency is much more common than toxicity, and it is quite common.
- A very small percentage of people have inherited a problem with zinc uptake and transport. However, about 2 billion people worldwide are affected by zinc deficiency from other causes.
- Symptoms of zinc deficiency include slowed growth and development, especially delayed puberty and adolescence, diarrhea, impotence, alopecia, skin rashes, acne, impaired wound healing, diminished appetite, impaired sense of taste and smell, night blindness, mood disorders, lower cognition, impaired immune function, especially in the at-risk populations such as children and older adults, poor carbohydrate utilization, diabetes, infertility, polycystic ovarian syndrome, and impaired methylation.
- Risk factors are those with poor dietary intake, malabsorption, such as celiac disease, short bowel syndrome, prolonged diarrhea, those with burns, especially severe burns, chronic kidney disease, inflammatory bowel diseases such as Crohn’s disease or ulcerative colitis, those on TPN, or total parenteral nutrition, liver disease and alcoholism, when it’s displaced by other heavy metals such an exposure to lead, like happened in Michigan in the United States a few years ago, older adults, vegetarians and vegans, premature or low-birth-weight infants, older breast-fed infants and toddlers without adequate access to zinc-rich foods, children and adolescents, pregnant and breast-feeding women, and especially teens and malnourished individuals, including those with anorexia.
- If someone has acute zinc toxicity, this could happen from food contamination when food is stored in galvanized containers and the zinc leaches into the food, this acute poisoning looks like severe abdominal pain, diarrhea, nausea, and vomiting. We actually have seen this with a single dose of anywhere between 225 and 450 milligrams of supplemental zinc when taken orally. Milder versions of these symptoms can be seen with doses of between 50 and 150 milligrams per day of supplemental zinc.
- Acute zinc toxicity could happen from inhalation of zinc oxide fumes. This is very rare but might result in fever, profuse sweating, weakness, and rapid breathing.
- Long-term consumption of excess zinc can result in copper deficiency. Zinc intake of about 60 milligrams per day combined as 50 milligrams of supplemental zinc plus 10 milligrams of dietary zinc for 10 weeks has been known to result in copper deficiency. Also be aware that use of intranasal zinc can lead to loss of sense of smell without recovery and should be avoided.
- How can zinc status be assessed? A clinician will assess a client for symptoms and risk of deficiency. Serum copper and plasma zinc can be measured via a blood test with a recommended balanced ratio of copper to zinc as 1 to 1.2 copper to 1 of zinc.
- Some clinicians assess clients with the Zinc Tally taste test that uses an oral liquid zinc test to assess for zinc status.
- A nutrition physical exam looks at fingernails for many small pinhead size white spots on fingernails that may indicate zinc deficiency. Also taking into account that damaged nails could have white spots as well.
- As a clinician, I will often assess zinc status in clients with fertility concerns, mood disorders, cognitive impairment, certain skin rashes, celiac disease, inflammatory bowel diseases, chronic diarrhea, and vegetarians and vegans.
BEST FOOD SOURCES
- Foods that are highest in zinc include oysters, red meat, cheese, crab, turkey, pork, and chicken.
- Foods with moderate amounts of zinc include soybeans, pinenuts, pumpkin seeds, cashews, yogurt, sunflower seeds, pecans, Brazil nuts, chickpeas, almonds, and baked beans.
- Zinc is actually high in many plant foods, but it’s tightly bound to phytic acid. A diet low in animal food and high in phytic acid found in plants is a risk factor for zinc deficiency. With proper preparation of zinc containing plant foods, zinc bioavailability can be increased. This population may need more zinc than the RDA values still, even with proper food preparation.
- Supplementation when zinc status needs to be corrected is possible. The first goal is resolution of signs and symptoms. Also, checking in with blood tests is recommended, including copper about every three months. You also want to identify the root cause. This should be addressed such as malabsorption.
- Supplemental forms of zinc include zinc acetate, gluconate, sulfate, citrate, or methionine. I do not recommend the use of zinc oxide or picolinate. Zinc carnosine is specific for healing the gut lining but is not well absorbed into the system.
- Zinc is best absorbed when taken 10 minutes before meals, but it can cause nausea in some people so it might need to be taken with food. The ideal dose that can be absorbed at any one time is about 10 to 15 milligrams of zinc combined with about 1 to 2 milligrams of copper taken one to three times a day, depending on severity of deficiency symptoms and tests.
- I like to use Jarrow Zinc Balance, as it has this optimal formula. However, if I’m assisting a client with copper overload or copper toxicity, I would choose a form of zinc supplementation that does not contain any copper.
- Be cautious about the amount of zinc taken via lozenges and in food, especially during cold and flu season. Cold or flu support is likely fine if limited in duration to no more than two weeks but is also dependent on food intake. An example is don’t eat a plate of oysters and take a lot of zinc supplements.
- There are some nutrient interactions to be aware of with zinc. Zinc certainly affects copper status. Taking too much zinc traps copper in the gut and prevents its absorption.
- Zinc increases the protection of metallothionein that binds copper.
- Some people have high copper that is associated with mental health conditions such as bipolar disorder, anxiety, or other mood disorders. Zinc can be carefully used to support lowering elevated copper with the guidance of a clinician.
- Iron and zinc compete for absorption pathways in the gut. So supplementing with iron may also risk lowering zinc levels.
- Other nutrients or food components may affect zinc absorption. This includes calcium supplementation and phytic acid. An example is pumpkin seeds. There are very good sources of zinc as pumpkin seeds, but a lot of it is bound to the phytic acid in the seeds. Eating pumpkin seeds that have been soaked, sprouted, and dried increases the bioavailability of the zinc.
- Folate production for methylation is also zinc dependent.
- Zinc and vitamin A also interact. Zinc is a component of the vitamin A transport protein. Zinc is a cofactor that helps convert vitamin A to its active form. Zinc deficiency is associated with decreased release of vitamin A from its storage site in the liver and may contribute to night blindness that is sometimes seen with zinc deficiency.